
Post-operative cardiac injury detection is becoming a critical challenge as cardiovascular care advances. Success is no longer defined strictly by survival on the operating table.
Today, the real challenge lies in the “blind spot” of the peri-operative window — what happens after the patient leaves the recovery room.
Recent data published in the European Heart Journal highlights a deeply uncomfortable truth: heart injury after non-cardiac surgery is common, frequently silent, and too often goes unnoticed unless a cardiologist is directly involved.
The Hidden Failure Behind “Successful” Procedures
Patients survive complex orthopaedic, oncological, or abdominal procedures. Their wounds heal, and by all visible measures, the surgery is a success.
And yet, in a significant proportion of these cases, Myocardial Injury after Non-cardiac Surgery (MINS) occurs without clear clinical signals.
Post-operative cardiac injury often presents:
- Without chest pain
- Without obvious ECG changes for general ward teams
- Without structured follow-up
These patients carry a substantially increased risk of:
- Heart failure
- Arrhythmias
- Rehospitalisation
- Premature mortality
Healthcare systems invest heavily in surgical pathways — yet lose value because cardiac injury is not identified when it is still manageable.
Why Post-Operative Cardiac Injury Detection Fails
In an ideal system, detection follows a clear sequence:
- Systematic troponin measurement
- Clinical escalation
- Cardiology involvement
- Timely echocardiography
In reality, this chain frequently breaks:
- Troponin is not measured routinely, or mild elevations are dismissed as “surgical stress”
- Echocardiography capacity is limited, with waiting lists extending weeks or months
- Symptoms are subtle or attributed to post-operative deconditioning
The result:
Patients with evolving ventricular dysfunction are missed.
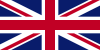
This gap in post-operative cardiac injury detection is illustrated below:
By the time they present with breathlessness or peripheral oedema, the system is no longer preventing damage — it is reacting to it.
Evidence of the “Invisible” Patient
Clinical observations and real-world experience reinforce this diagnostic gap.
Even among patients already under cardiovascular care, cases of previously unrecognised heart failure and ventricular dysfunction continue to emerge when more advanced functional assessment is applied.
These are not “lost” patients.
They are already within the healthcare system — yet their condition remains undetected.
When we fail to look, we fail to find.
A Scalable Triage Layer: Where Cardio-HART™ Fits
Cardio-HART™ is not designed to replace echocardiography.
Instead, it introduces a scalable, point-of-care triage layer for post-operative cardiac injury detection.
By combining:
- ECG
- Phonocardiography
- Echo-equivalent bio-signal analysis
Cardio-HART enables detection of cardiac dysfunction, including:
- Reduced ejection fraction
- Heart failure phenotypes
- Structural and functional abnormalities
- Valvular disease indicators
This allows clinicians to move beyond symptom-based assessment and introduce objective functional screening earlier in the patient pathway.
The key clinical question is not:
“Can this replace echocardiography?”
But rather:
“Can we identify which patients need it — earlier?”
The Economic and Ethical Imperative
The impact of missed post-operative cardiac injury extends beyond clinical outcomes.
A reactive pathway leads to:
- Delayed diagnosis
- Emergency admissions
- Increased long-term treatment burden
A proactive approach enables:
- Earlier detection
- Timely treatment initiation
- More efficient use of cardiology resources
- Reduced unnecessary referrals and readmissions
This is not only clinically meaningful — it is operationally and economically rational.
Ethically, the case is even stronger.
Patients do not consent to:
- Silent myocardial damage
- Preventable heart failure
- Diagnostic delays caused by system limitations
When evidence shows these injuries are common and frequently overlooked, inaction becomes increasingly difficult to justify.
A Call to Proactive Cardiology
To protect surgical outcomes, post-operative cardiac injury detection must evolve.
This includes:
- Structured cardiac assessment before discharge in high-risk surgeries
- Follow-up functional screening within the 2–6 week window
- Objective referral thresholds based on measurable data
- Integration of scalable diagnostic technologies to reduce echocardiography bottlenecks
Cardiology can no longer remain reactive.
It must become proactive — supported by tools that make early detection operationally possible.
Meet Us in Turkey
We will be attending the 34th ANNUAL MEETING OF ASCVTS in Antalya.
Visit us at Stand 38
Let’s discuss how post-operative cardiac injury detection can be integrated into real clinical pathways — and what it means for the future of cardiovascular outcomes.