
Why ECG Misses Heart Failure — and How Echo-Equivalent Diagnostics Improve
Early Detection
In primary care, cardiovascular disease (CVD), heart failure (HF), and valvular heart disease (VHD) are often first evaluated using a 12-lead ECG. While ECG is essential for rhythm assessment, it does not directly assess structural or functional cardiac abnormalities — the defining features of most heart failure and valve diseases.
A “normal ECG” does not rule out heart disease.
Most clinicians know that.
And yet, ECG is still used as a gatekeeper in primary care.
As a result, clinically significant pathology may remain undetected until echocardiography becomes available through referral pathways.
This page is the clinical background behind two related articles:
- Read the case: A True Story: When Heart Failure Missed by ECG Confronts the Rent
- Read the commentary: ECG Is Failing Us — and Guidelines Already Know It
This page explains:
What ECG Measures — and What It Does Not
What ECG Is Strong At
- Rhythm assessment (e.g., atrial fibrillation)
- Conduction abnormalities
- ST-T changes suggestive of ischemia
- Some electrical criteria suggestive of hypertrophy
What ECG Does Not Directly Measure
- Left ventricular ejection fraction (LVEF)
- Structural enlargement (atria or ventricles)
- Diastolic dysfunction
- Valve stenosis or regurgitation
- Pulmonary hypertension
Most heart failure phenotypes — HFpEF, HFmrEF, and HFrEF — are defined by structural and functional abnormalities, not electrical ones.
ECG may appear “normal” or inconclusive even when clinically significant heart disease is present.
Why ECG Misses Heart Failure in Primary Care
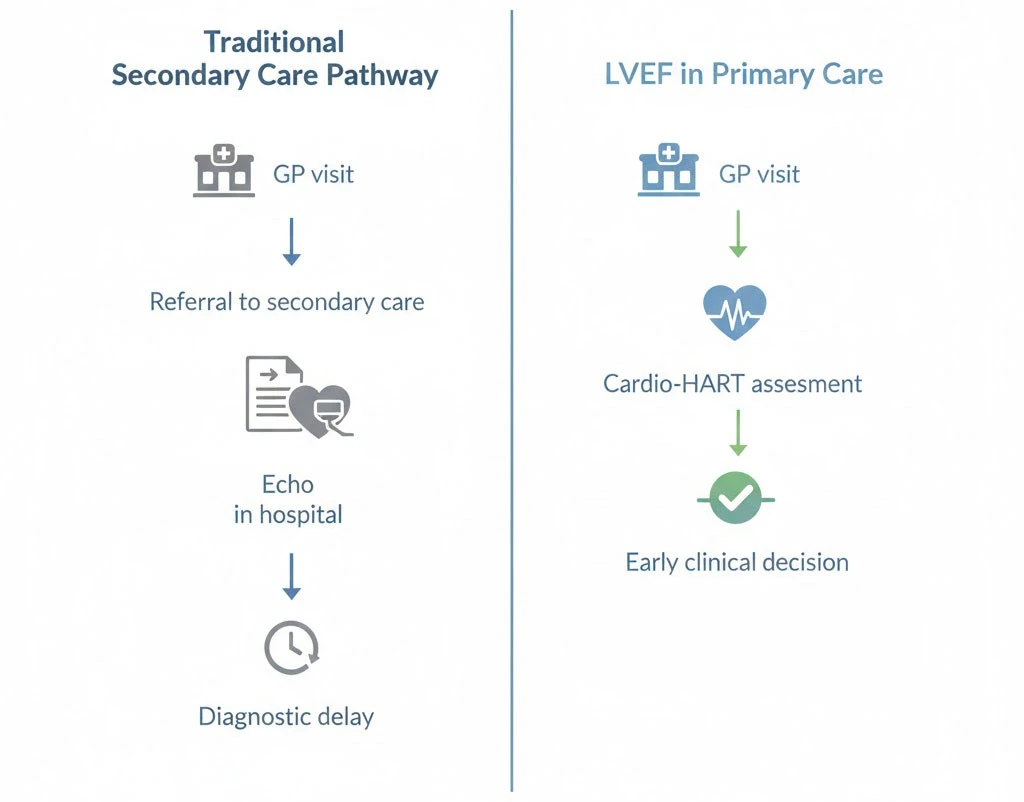
Echocardiography is the reference standard for diagnosing structural heart disease, functional impairment, valve abnormalities, and reduced LVEF.
However, echocardiography is not typically available at first presentation in primary care. It requires referral to secondary care, often associated with waiting times measured in months.
ECG is accessible but incomplete.
Echocardiography remains the reference standard, but access is often gated by waiting times that can exceed eight months—as seen in recent clinical cases where urgent pathology was classified as routine.
This gap was illustrated in a real clinical encounter at ESC Congress Madrid 2025, where ECG findings appeared non-urgent while echo-equivalent findings indicated severe structural and functional dysfunction — and the report was later dismissed because it did not fit standard pathways.
Cardio-HART: Echo-Equivalent Diagnostics at Point of Care
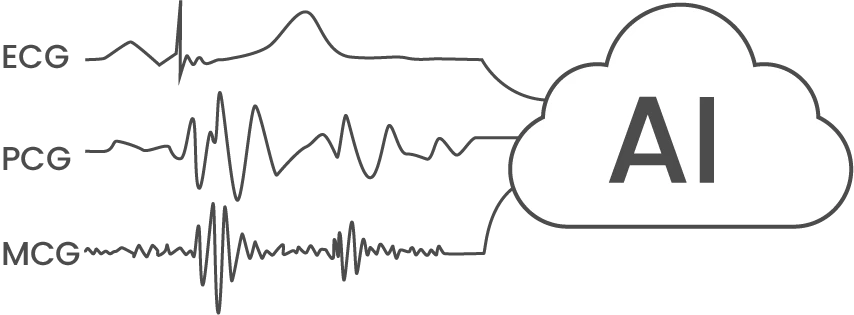
Cardio-HART’s ‘echo-equivalent’ findings are generated by proprietary AI models that perform a synchronous multi-modal analysis of ECG, PCG, and MCG bio-signals. By correlating electrical, acoustic, and mechanical cardiac data, the system identifies structural and functional indicators that are traditionally only visible via echocardiography.
Cardio-HART™ (CHART) is an AI-enabled cardiac diagnostic system that combines:
- 12-lead ECG
- Phonocardiography (PCG)
- Mechano-cardiography (MCG)
Using novel bio-signals and AI models, Cardio-HART predicts 14 structural and functional abnormalities typically diagnosed by echocardiography and reports them as HART-findings with severity indication.
Structural & Functional Findings
- Left ventricular hypertrophy (LVH)
- Dilated cardiomyopathy (DCM)
- Atrial enlargement (LAE, RAE)
- Right ventricular enlargement (RVE)
- Systolic and diastolic dysfunction
- Wall motion abnormalities
Valve & Pressure Findings
- Aortic stenosis / regurgitation
- Mitral stenosis / regurgitation
- Tricuspid regurgitation
- Pulmonary hypertension
Cardio-HART also estimates LVEF, classifies heart failure phenotype, and provides an HF-score to support clinical decision-making.
The test captures three one-minute recordings and generates results within minutes, using ECG, PCG, and MCG bio-signals to produce echo-equivalent structural and functional findings.
Detection of All Three Heart Failure Phenotypes
Heart failure is categorized by LVEF:
HFpEF
Preserved EF (≥50%)
HFmrEF
Mildly reduced EF (40–49%)
HFrEF
Reduced EF (<40%)
Standard ECG cannot estimate LVEF. Cardio-HART provides estimated LVEF and phenotype classification at the point of care.
Clinical Performance Summary
Cardio-HART has been clinically validated against echocardiography.
| Heart Failure Detection | Functional Heart Disease |
| Sensitivity: 83.7% | Sensitivity: 90.7% |
| Specificity: 89.3% | Specificity: 90.9% |
| AUC: 92.7% | AUC: 96.4% |
| Valvular Heart Disease | Abnormal Echo |
| Sensitivity: 84.1% | Sensitivity: 87.6% |
| Specificity: 89.8% | Specificity: 85.7% |
Where Cardio-HART Fits in Clinical Practice
Primary Care
First presentation of dyspnea, fatigue, palpitations
Heart Failure Clinics
Monitoring structural and functional progression
Emergency Departments
Rapid triage support
Secondary Care
Referral prioritization support
Regulatory & Clinical Status
- CE-marked (MDR Class IIa device) & FDA 510(k) clearance (K182970).
- ISO 13485-certified QMS; GDPR / HIPAA compliant cloud.
- NHS Digital Technology Assessment Criteria (DTAC) Green Pass – June 2025.
- Annual NB audits (SIQ Slovenia) and Cyber Essentials certified.
Cardio-HART does not replace echocardiography when echocardiography is indicated. Final diagnosis remains with the clinician.

If you want the full clinical argument about ECG overreliance and why pathways reject innovation, read: ECG Is Failing Us — and Guidelines Already Know It.
Book a Clinical Demonstration
See how Cardio-HART integrates into primary care workflow and supports heart failure and valve disease detection at first presentation.